
Visualization of Dynamic Expression of Myocardial Sigma-1 Receptor After Myocardial Ischemia and Reperfusion Using Radioiodine-Labeled 2-[4-(2-iodophenyl)piperidino]cyclopentanol (OI5V) Imaging
![Visualization of Dynamic Expression of Myocardial Sigma-1 Receptor After Myocardial Ischemia and Reperfusion Using Radioiodine-Labeled 2-[4-(2-iodophenyl)piperidino]cyclopentanol (OI5V) Imaging](https://advantx.org/wp-content/uploads/2022/06/young-mixed-race-doctor-in-uniform-looking-at-pati-2021-09-24-03-24-01-utc-scaled-1100x550.jpg)
By Hiroshi Wakabayashi, Junichi Taki, Hiroshi Mori, Tomo Hiromasa, Norihito Akatani, Anri Inaki, Takashi Kozaka, Kazuhiro Shiba, Kazuma Ogawa, Seigo Kinuya
Excerpt from the article published in Circulation Journal, Article ID CJ-21-0320, Online ISSN 1347-4820, Print ISSN 1346-9843, DOI: https://doi.org/10.1253/circj.CJ-21-0320
Editor’s Highlights
- The sigma-1 receptor chaperone (σ1R) is considered as a pluripotent modulator with resultant multiple functional manifestations in the living system.
- σ1R is also expressed in cardiomyocytes as a chaperon and regulates the response to ER stress, modulates calcium handling, and affects the function of voltage-gated-ion channels in abnormal states.
- σ1R has been found in cardiomyocytes, where it was documented to play a role in contractility and beating frequency.
- ER stress plays an essential role in developing and progressing cardiovascular disease.
- σ1R is downregulated in cardiomyocytes following heart failure.
- The modulation of the σ1R signal with ligands was implicated in cardioprotection.
- σ1R has been found to act as a pluripotent modulator in various conditions, including ischemia.
- Visualization of σ1R expression, radiolabeled OI5V imaging may be a non-invasive way to monitor myocardial injury and its ER stress after ischemia and reperfusion
Abstract
Background: This study chronologically evaluated the expression of the intensity and distribution of the sigma-1 receptor (σ1R) demonstrated by radiolabeled 2-[4-(2-iodophenyl)piperidino]cyclopentanol (OI5V) in a rat model of myocardial ischemia and reperfusion.
Methods and Results: The left coronary artery was occluded for 30 min, followed by reperfusion. Dual-tracer autoradiography with 125I-OI5V and 99 mTc-MIBI was performed to assess the spatiotemporal changes in 125I-OI5V uptake (n=5–6). Significant and peaked 125I-OI5V uptake in the ischemic area was observed at 3 days after reperfusion, and the 125I-OI5V uptake ratio of ischemic area to normally perfused left ventricular area decreased gradually from 3 to 28 days (mean value±SD; 0.90±0.12 at 1 day, 1.89±0.19 at 3 days, 1.52±0.17 at 7 days, 1.34±0.13 at 14 days, and 1.16±0.14 at 28 days, respectively). Triple-tracer autoradiography with 125I-OI5V, 99 mTc-MIBI, and 201TlCl was performed to evaluate 125I-OI5V uptake in the ischemic area in relation to the residual perfusion at 7 days (n=4). The 125I-OI5V uptake ratio of the non-salvaged area was higher compared to that of the salvaged area in the ischemic area. 123I-OI5V and 99 mTc-MIBI SPECT/CT was performed 3 days after reperfusion (n=3), and the in vivo images showed clear uptake of 123I-OI5V in the perfusion defect area.
Conclusions: The present study confirmed the spatiotemporal expression pattern of σ1R expression. Non-invasive σ1R imaging with 123I or 125I-OI5V was feasible to monitor the expression of σ1R after myocardial ischemia and reperfusion.
Introduction
Sigma receptor was first recognized as an opioid receptor subtype in the 1970s,1 and was later reclassified as a unique receptor due to its different properties.2 Two subtypes of sigma receptor (sigma-1 and -2 receptor) have been identified,3 and the sigma-1 receptor (σ1R) was first cloned in 1996 from guinea pig liver.4 The σ1R primarily resides at the endoplasmic reticulum (ER) membrane associated with mitochondria (MAM) and is also translocated to the plasma membrane under stress. It acts as a chaperone that regulates protein folding / degradation, ER / oxidative stress, and cell survival.5 It is considered as a pluripotent modulator with resultant multiple functional manifestations in the living system.6 It has been intensively studied in the central nervous system thus far and has been implicated in many diseases, including schizophrenia, clinical depression, Alzheimer’s disease, Parkinson’s disease, cocaine addiction, stroke/ischemia, myocardial hypertrophy, and cancer.7,8
In the heart, σ1R is also expressed in cardiomyocytes as a chaperon and regulates the response to ER stress, modulates calcium handling, and affects the function of voltage-gated-ion channels in abnormal states.5 The σ1R knockout mouse model demonstrated cardiac dysfunction with mitochondrial dysfunction, abnormal mitochondrial architecture, and adverse cardiac remodeling.9 The σ1R contributed to understanding the pathophysiology of myocardial hypertrophy. In transverse aortic constriction (TAC) mice, σ1R is downregulated in cardiomyocytes following heart failure;10 however, the spatiotemporal expression patterns of σ1R after myocardial ischemia and reperfusion have not been explored.
A radiotracer 125I-2-[4-(2-iodophenyl)piperidino]cyclopentanol (OI5V), vesamicol analog with 5-membered ring structure, shows a high selective binding affinity for σ1R. 125I-OI5V is a promising candidate for a σ1R imaging probe.11 The use of hybrid imaging devices such as single-photon emission computed tomography (SPECT) with computed tomography (CT) enables non-invasive imaging of σ1R distribution in preclinical and human subjects. Here, we evaluated the spatiotemporal changes in the intensity of the expression of σ1R demonstrated by OI5V radiolabeled with 123I or 125I in a rat model of ischemia and reperfusion.
…
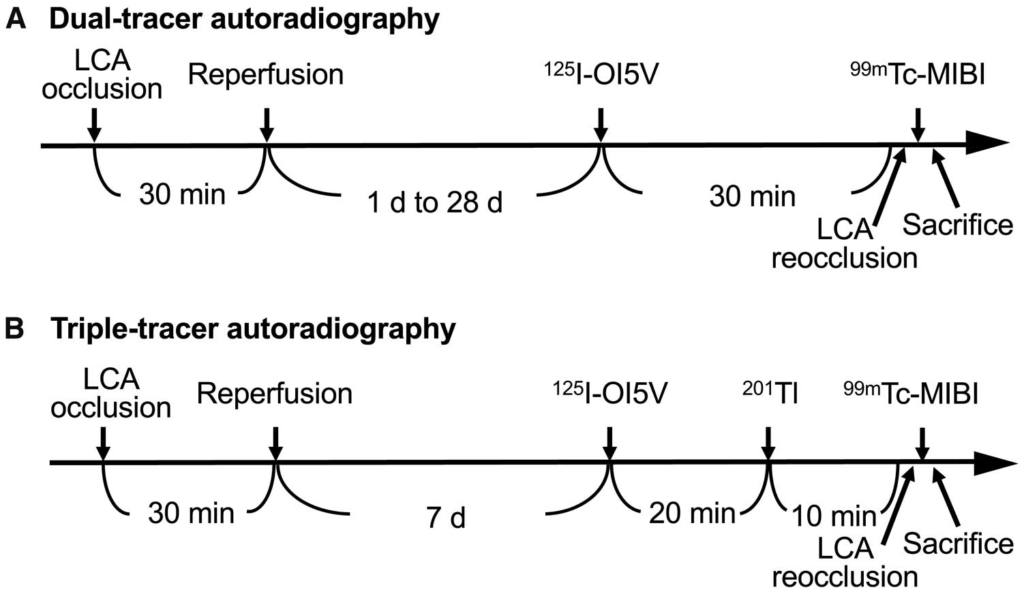
Autoradiography protocol for the rat model of 30 min ischemia and reperfusion.
(A) The left coronary artery (LCA) was occluded for 30 min, followed by reperfusion. At 1, 3, 7, 14, and 28 days after 30 min ischemia and reperfusion, 125I-OI5V was injected via a tail vein. Thirty min after the tracer injection, 99 mTc-MIBI was injected just after reocclusion of the proximal portion of the LCA for delineation of the ischemic area in dual-tracer autoradiography. (B) In triple-tracer autoradiography, an additional 201Tl was injected for the myocardial perfusion image 20 min after the 125I-OI5V injection. MIBI, hexakis 2-methoxyisobutyl isonitrile; OI5V, 2-[4-(2-iodophenyl)piperidino]cyclopentanol.
…
Results
Dual-Tracer Autoradiography
Autoradiography showed homogeneous 125I-OI5V uptake in the myocardium in healthy rat hearts (n=2). Perfusion defects and focal 125I-OI5V uptake were not observed in the sham-operated rats (n=4).
The area of increased 125I-OI5V uptake was localized in the area of ischemia (area at risk), as shown by 99 mTc-MIBI uptake defect. No significant elevation of 125I-OI5V uptake was found in the non-ischemic area, identified by 99 mTc-MIBI. At 1 day after ischemia and reperfusion, a 125I-OI5V image demonstrated reduced tracer activity in the area at risk compared to the normally perfused area; however, 125I-OI5V uptake increased significantly and peaked at 3 days after ischemia and reperfusion followed by gradual reduction until 28 days (Figure 2A). The 125I-OI5V uptake ratios of ischemic area to normal perfusion LV area were 0.90±0.12 at 1 day, 1.89±0.19 at 3 days, 1.52±0.17 at 7 days, 1.34±0.13 at 14 days, and 1.16±0.14 at 28 days (Figure 2B). The ratio of 125I-OI5V uptake area to the ischemic area was 0±0 at 1 day, 0.54±0.09 at 3 days, 0.52±0.04 at 7 days, 0.44±0.10 at 14 days, and 0.44±0.06 at 28 days. The ratio of 125I-OI5V uptake area in the ischemic area did not change from 3 to 28 days. The blocking study with (+/−)-pentazocine showed a marked reduction of 125I-OI5V uptake at 3 days from 1.89±0.20 to 1.13±0.18 (P<0.05, Figure 3).
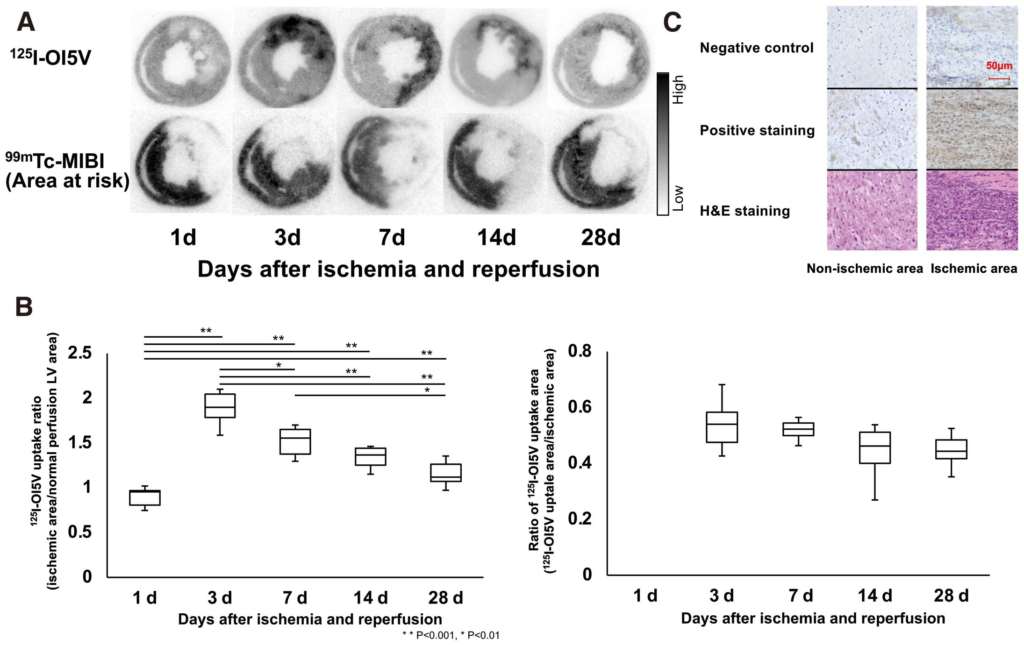
(A) Corresponding dual-tracer autoradiographic short-axis images in rats after ischemia and reperfusion (125I-OI5V and 99 mTc-MIBI). (B) Time course of 125I-OI5V uptake ratio of ischemic area to remote uptake after coronary occlusion and reperfusion. 99 mTc-MIBI images demonstrate the ischemic area because the tracer was injected during coronary reocclusion before sacrifice. Box and whisker plot show the range from 25% to 75%. The median value is indicated with a horizonal bar, and the whiskers indicate the upper and lower limits. Intense 125I-OI5V uptake was observed in the ischemic area at 3 days after ischemia and reperfusion. The increase of tracer signal in the ischemic area peaked at 3 days, followed by a gradual reduction of uptake until the 28th day. The ratio of 125I-OI5V uptake area in the ischemic area did not change from 3 to 28 days. (C) Immunohistochemical staining (brown) showed an increased Sigma-1 receptor in the ischemic area at 3 days after ischemia and reperfusion. MIBI, hexakis 2-methoxyisobutyl isonitrile; OI5V, 2-[4-(2-iodophenyl)piperidino]cyclopentanol.
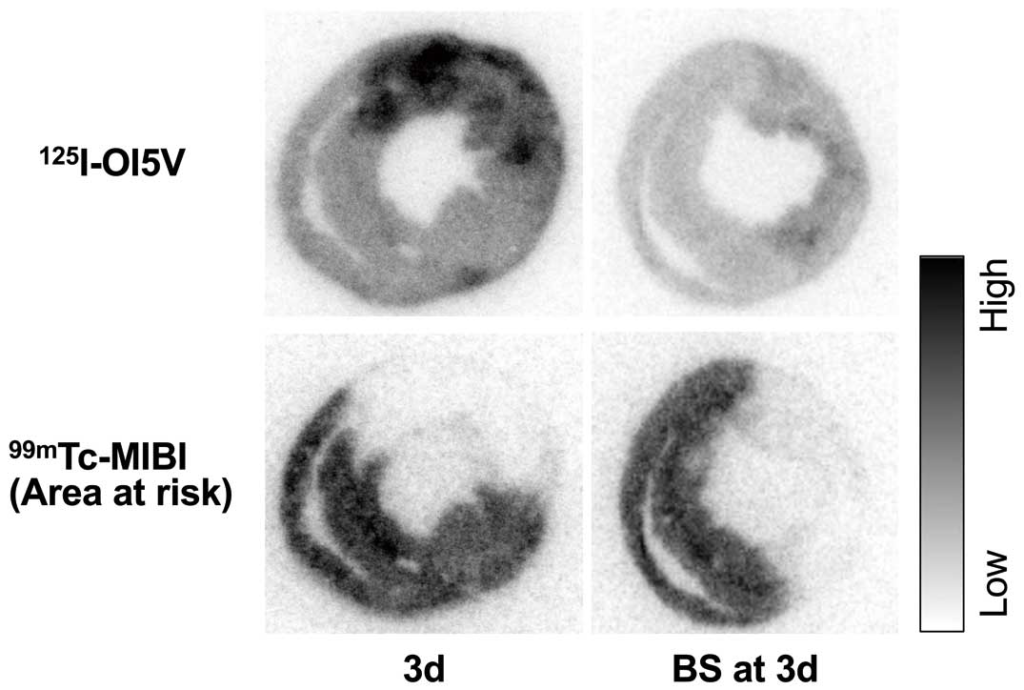
Dual-tracer autoradiographic short-axis images in the blocking study. The blocking study with (+/−)-pentazocine showed a significant reduction of 125I-OI5V concentration at 3 days after ischemia and reperfusion. BS, blocking study; MIBI, hexakis 2-methoxyisobutyl isonitrile; OI5V, 2-[4-(2-iodophenyl)piperidino]cyclopentanol.
Immunohistochemical Analysis
Significant immunohistochemical staining showed an increased σ1R on the myocardium in the ischemic area (area at risk) at 3 days after ischemia and reperfusion (Figure 2C).
Triple-Tracer Autoradiography
125I-OI5V uptake was observed in both the salvaged and non-salvaged areas of the ischemic area at 7 days after ischemia and reperfusion (Figure 4), whereas no significant regional elevation of 125I-OI5V uptake was found in the non-ischemic area. The salvaged area was observed in 67±13% of the ischemic area (area at risk). The 125I-OI5V uptake ratio of the non-salvaged area was higher compared to that of the salvaged area (2.11±0.30 vs. 1.46±0.14, P<0.01).
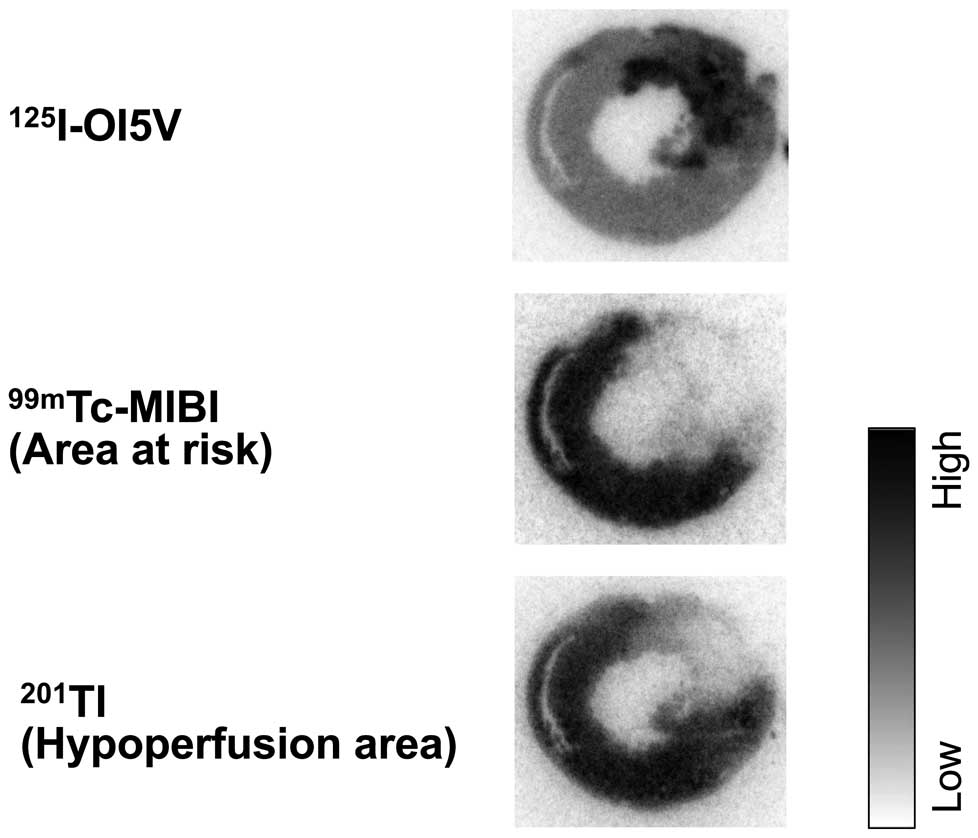
Corresponding triple-tracer autoradiographic short-axis images in rats after ischemia and reperfusion (125I-OI5V, 99 mTc-MIBI, and 201Tl). 99 mTc-MIBI and 201Tl images demonstrate ischemic area (area at risk) and the hypoperfusion area, respectively. Intense 125I-OI5V uptake was observed predominantly in the non-salvaged ischemic myocardium, but mild uptake was also observed in the salvaged area at 7 days after ischemia and reperfusion. MIBI, hexakis 2-methoxyisobutyl isonitrile; OI5V, 2-[4-(2-iodophenyl)piperidino]cyclopentanol.
Systemic 125I-OI5V Distribution
In vivo biodistribution was evaluated at 30 min after 125I-OI5V administration. The lung, kidney, pancreas, and intestine exhibited high tracer concentration, and tracer uptake in the blood remained very low. Tracer uptake in the cardiac ischemic area was higher in rats with an ischemia and reperfusion model compared with that of sham-operated rats. In the non-ischemic area, tracer uptake tended to be higher after the ischemia and reperfusion. The results of the post mortem tissue counting study are summarized in Table.
Table. Postmortem Tissue Counting in Rats at 30 min After Injection of 125I-OI5V
| Organ | Uptake (%ID/g)† | P value | |
|---|---|---|---|
| Sham-operated rats | Rats with ischemia and reperfusion | ||
| Blood | 0.08±0.01 | 0.07±0.01 | NS |
| Lung | 3.53±0.80 | 3.74±0.80 | NS |
| Heart | |||
| Non-ischemic area | 0.53±0.06 | 0.62±0.03 | NS |
| Ischemic area (operated area) | 0.53±0.03 | 1.76±0.37 | <0.0001 |
| Liver | 1.38±0.15 | 1.18±0.15 | NS |
| Kidney | 1.96±0.14 | 2.10±0.14 | NS |
| Spleen | 1.62±0.11 | 1.67±0.11 | NS |
| Pancreas | 2.66±0.39 | 2.44±0.32 | NS |
| Stomach | 1.03±0.25 | 0.67±0.25 | NS |
| Intestine | 2.18±0.66 | 2.02±0.66 | NS |
| Muscle | 0.10±0.01 | 0.12±0.01 | 0.03 |
| Bone | 0.33±0.01 | 0.36±0.01 | NS |
†Uptake values are presented as mean percentage of the injection dose per gram of tissue (%ID/g)±standard deviation. NS, not significant.
In Vivo SPECT/CT Imaging
Focally increased 123I-OI5V uptake in the myocardium was clearly observed in the hypoperfused area showing reduced 99 mTc-MIBI uptake at 3 days after ischemia and reperfusion (Figure 5). The mean count ratio of the decreased perfusion area to the preserved perfusion area was 2.0±0.2 at 3 days after ischemia and reperfusion (n=3).
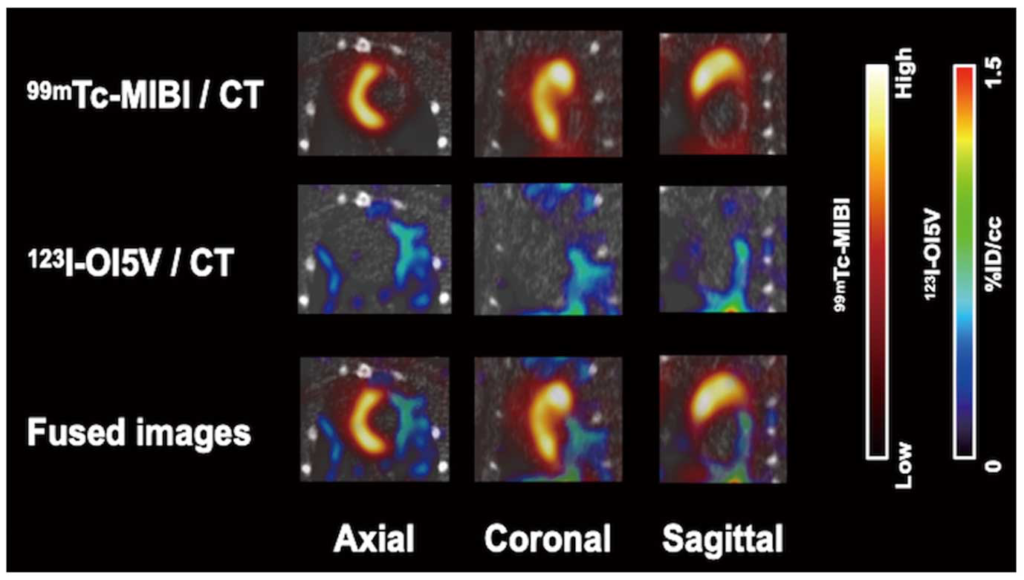
In vivo 99 mTc-MIBI and 123I-OI5V SPECT/CT images of rats at 3 days after ischemia and reperfusion. Axial, coronal, and sagittal views showing focal increased 123I-OI5V uptake in areas of reduced myocardial perfusion by 99 mTc-MIBI. MIBI, 99 mTc-hexakis 2-methoxyisobutyl isonitrile; OI5V, 2-[4-(2-iodophenyl)piperidino]cyclopentanol.
Discussion
The present study demonstrated the feasibility of imaging with OI5V targeted at the σ1R, and documented, for the first time, spatiotemporal profiling of σ1R expression after myocardial ischemia and reperfusion. We surmise that in the model of ischemia and reperfusion, ischemia is the major factor determining the degree of σ1R expression, in that the 125I-OI5V uptake was higher in the non-salvaged area than the salvaged area. Furthermore, 125I-OI5V imaging revealed that the σ1R expression changes dynamically after ischemia and reperfusion.
σ1R has been found in cardiomyocytes, where it was documented to play a role in contractility and beating frequency.16,17 σ1R ligands, agonists or antagonists have been applied to observe the downstream effects to elucidate the mechanism of its action in the heart. σ1Rs as chaperones have been shown to be involved in ER stress, calcium handling, voltage-gated ion channeling, cellular toxicity/apoptosis, and hypertrophy.5,18 Here, the modulation of the σ1R signal with ligands was implicated in cardioprotection. However, the possible involvement of σ1R expression in the pathophysiological process has not yet been examined in ischemic heart disease, though ischemia and reperfusion injury trigger calcium imbalance, ER stress, and apoptosis.19 The current study confirms that σ1R overexpression occurs shortly after ischemia and reperfusion.
σ1R has been found to act as a pluripotent modulator in various conditions, including ischemia.18 Our imaging study is in line with prior studies showing the presence of σ1R under ischemia in the brain of mice with permanent middle cerebral artery occlusion,20 in which σ1R expression increased in the peri-infarcted area at 1 week after infarction. However, its chronological changes and distribution in the brain are unknown. We here clarified the spatiotemporal σ1R expression in the damaged heart after ischemia and reperfusion.
In the autoradiographic study, significant σ1R expression was observed in the myocardium within the ischemic area, with the expression peaking at 3 days, followed by a gradual reduction to 28 days. At 3 days after ischemia and reperfusion, we also confirmed the presence of σ1R in the ischemic area by immunostaining, a high tracer signal in the ischemic area by postmortem tissue counting, and the significant reduction of the tracer signal by a blocking study. σ1R is an ER protein that primarily resides specifically in the mitochondria-associated ER membrane; however, it can be translocated to the plasma membrane, mitochondria, nucleus envelope and cytosol, and functions as the chaperone during various increasing cellular stresses.5,6,17 Based on the presence of σ1R under stress, the 125I-OI5V uptake demonstrated by autoradiography may correspond to the upregulated σ1R in the cardiomyocytes after ischemia and reperfusion.
The current study demonstrated the inhomogeneous expression of 125I-OI5V in the ischemic area regardless of the salvage status. The triple autoradiography showed higher 125I-OI5V uptake in the non-salvage area compared with the salvaged area in the ischemic region. The discordant 125I-OI5V uptake in the decreased perfusion area may reflect the presence of residual myocardium jeopardized by more severe ischemia. In response to severe ischemia, cardiomyocytes increase the expression of various chaperones and activities as a salvage mechanism to manage emergency conditions.21 If a more intense expression of σ1R reflects more severe ischemic damage in viable myocardium, σ1R imaging could embody the concept of the stress imaging, reflecting prior damage or current stress.
ER stress plays an essential role in developing and progressing cardiovascular disease.22,23 We speculated that σ1R imaging also might be beneficial in non-ischemic heart disease such as myocardial hypertrophy due to TAC; the σ1R was gradually downregulated along with ventricular dysfunction.10,18,24 In such a condition, the tracer uptake in the heart might decrease. For the evaluation of σ1R downregulation, absolute quantification of the tracer uptake should be important.
The OI5V was radiolabeled with radioiodine so that the radioactivity would reveal the in vivo dynamics of σ1R expression. The average 123I-OI5V count ratio in in vivo SPECT/CT is similar to the average ratio of the ischemic area to normal LV area obtained from the 125I-OI5V autoradiography study. For future clinical application as a SPECT, 123I-OI5V would be beneficial to monitor and clarify how σ1R is involved pathophysiologically in the period of post myocardial infarction induced by ischemia and reperfusion. However, in the interpretation of inferior myocardial uptake, we must take into consideration the effect of relatively high liver uptake.
Conclusions
The present study demonstrated the feasibility of targeted imaging for serial assessment of regional expression of σ1R after myocardial ischemia and reperfusion. It also demonstrated the expression pattern in relation to myocardium perfusion status after 30 min of ischemia and reperfusion. The data from this study implied that, by allowing visualization of σ1R expression, radiolabeled OI5V imaging may be a non-invasive way to monitor myocardial injury and its ER stress after ischemia and reperfusion.