
Impact of history of mental disorders on short-term mortality among hospitalized patients with sepsis: A population-based cohort study
By Lavi Oud, and John Garza
Excerpt from the article published in PLoS ONE 17(3): e0265240. Published: March 10, 2022, DOI: https://doi.org/10.1371/journal.pone.0265240
Editor’s Highlights
- Sepsis remains a major global health burden with estimated nearly 49 million cases worldwide in 2017 and 11 million sepsis-related deaths.
- Mental disorders were associated, unexpectedly, with markedly lower risk of short-term mortality in sepsis.
- Fluvoxamine is a selective serotonin reuptake inhibitor and a strong agonist of sigma-1-receptor, a resident chaperone protein in the endoplasmic reticulum (ER).
- Relatively limited preclinical evidence suggests potentially beneficial effects of psychotropic agents in sepsis.
Abstract
Background: Mental disorders are associated with markedly reduced life expectancy, in part due to an increased risk of death due to infection, likely reflecting sepsis-associated mortality. Patients with mental disorders are at an increased risk of sepsis, but data on the prognostic impact of mental disorders in sepsis are sparse, showing conflicting findings.
Methods: We used statewide data to identify hospitalizations aged ≥18 years with sepsis in Texas during 2014–2017. Mental disorders, including mood, anxiety, psychosis, and personality disorders were identified using Clinical Classification Software codes. Multilevel, multivariable logistic regression with propensity adjustment (primary model), with propensity score matching, and multivariable logistic regression as alternative models, were used to estimate the association between mental disorders and short-term mortality (defined as in-hospital mortality or discharge to hospice). Additional models were fitted for sensitivity analyses and to estimate the prognostic associations of individual categories of mental disorders.
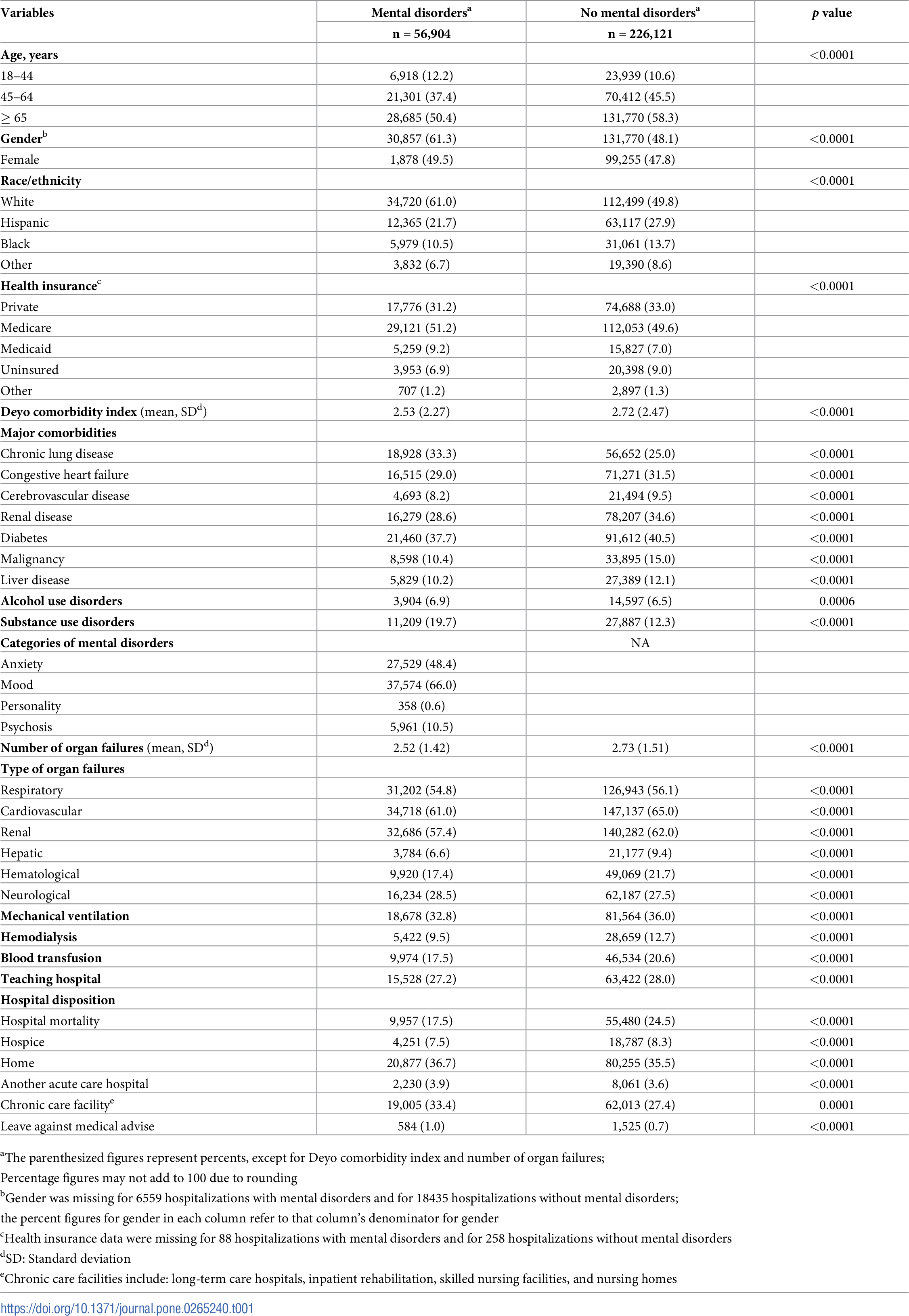
Results: Among 283,025 hospitalizations with sepsis, 56,904 (20.1%) had mental disorders. Hospitalizations with vs without mental disorders were younger (age 18–44 years 12.2% vs 10.6%), more commonly white (61.0% vs 49.8%), with lower burden of comorbidities (mean [SD] Deyo comorbidity index 2.53 [2.27] vs 2.73 [2.47]), and with lower need for organ support (mechanical ventilation 32.8% vs 36.0%); p<0.0001 for all comparisons. Crude short-term mortality among sepsis hospitalizations with and without mental disorders was 25.0% vs 32.8%, respectively. On adjusted analyses, mental disorders remained associated with lower odds of short-term mortality (adjusted odds ratio 0.792 [95% CI 0.772–0.812]). This finding was consistent on the alternative modeling approaches, sensitivity analyses, and examination of individual categories of mental disorders.
Conclusions: Mental disorders were associated, unexpectedly, with markedly lower risk of short-term mortality in sepsis. Further studies to examine the mechanisms underlying these findings may inform future efforts to improve sepsis outcomes.
Introduction
Sepsis remains a major global health burden with estimated nearly 49 million cases worldwide in 2017 and 11 million sepsis-related deaths [1]. Despite improving sepsis-associated mortality over the past decades [2, 3], attributed in part to care improvements, considerable outcome disparities remain among affected patients [1, 4, 5]. A more comprehensive understanding of the conditions associated with increased mortality in septic patients can inform targeted policy- and clinical practice-related preventive and interventional efforts. Contemporary efforts to improve sepsis outcomes have focused mostly on outcome disparities associated with sociodemographic traits (e.g., race [4]) and pre-existing “physical” illness (e.g., cancer [5]).
Mental disorders are highly prevalent, estimated to affect over 970 million people worldwide in 2017 [6], and are increasingly recognized as the major contributor to years lived with disability [7]. Crucially, mental disorders shorten life expectancy by 11–20 years [8], primarily due to natural causes, with 2.2-fold higher risk of all-cause mortality compared to the general population [9], resulting in approximately 8 million attributable deaths per year worldwide [9]. The mechanisms underlying the shortened life expectancy in affected patients are not completely understood, but the increased risk of mortality is thought to be related to prevalent risky lifestyle choices, altered engagement with the health care system, increased risk of comorbid conditions, and poorer quality of preventive and interventional medical care [10]. In 2019, only 44.8% of adults with mental disorders in the United States received mental health services within the preceding 12 months [11], with markedly lower rates in lower-resource countries [12].
Infections are one of the causes of reduced life expectancy in patients with mental disorders, with 1.9 to 5.2-times higher risk of death due to an infection, compared to the general population [8], with sepsis considered the major cause of death from infectious diseases [1, 13]. The increased risk of infection-related deaths among patients with mental disorders may represent higher risk of infection and sepsis, increased case fatality among septic patients, or a combination of both. Distinction between these possibilities is important, as it would guide different interventions. Numerous studies have linked mental disorders with increased risk of infection [14–17] and sepsis [15, 17, 18]. On the other hand, data on the prognostic impact of mental disorders in sepsis are sparse and show mixed findings.
Two recent population-based reports from Denmark, studying outcomes of hospitalizations with an infection found increased 30-day mortality among the subgroup with sepsis among patients who had mental disorders, compared to those without mental disorders [19, 20]. Although the specific causes of the poorer outcomes among septic patients with mental disorders were unclear, the investigators hypothesized that poor self-care, lower adherence to therapy of chronic medical conditions, higher burden of physical comorbidities, and differences in preventive and inpatient care may have played a role [19, 20]. On the other hand, in three other population-based studies from Germany [21] and the United States [22, 23] that sought to examine potential prognostic factors in severe sepsis and septic shock, presence of depression or psychosis were each associated with lower risk of death. None of these latter studies focused specifically on the findings related to mental disorders. The sources of the conflicting findings between these studies are unclear. In addition, comparisons between these reports and the generalizability of their findings are further constrained by lack of reported data on the characteristics and mortality rates of septic patients with and without mental disorders in these studies [19–23].
Because mental disorders remain a major global health burden, a better understanding of their prognostic role in sepsis can inform health policy, resource allocation, and targeted efforts to improve sepsis outcomes in this population. Here, we report a population-based study of adult hospitalizations with sepsis, seeking to examine the association of mental disorders with short-term mortality. We hypothesized that mental disorders are associated with increased risk of death.
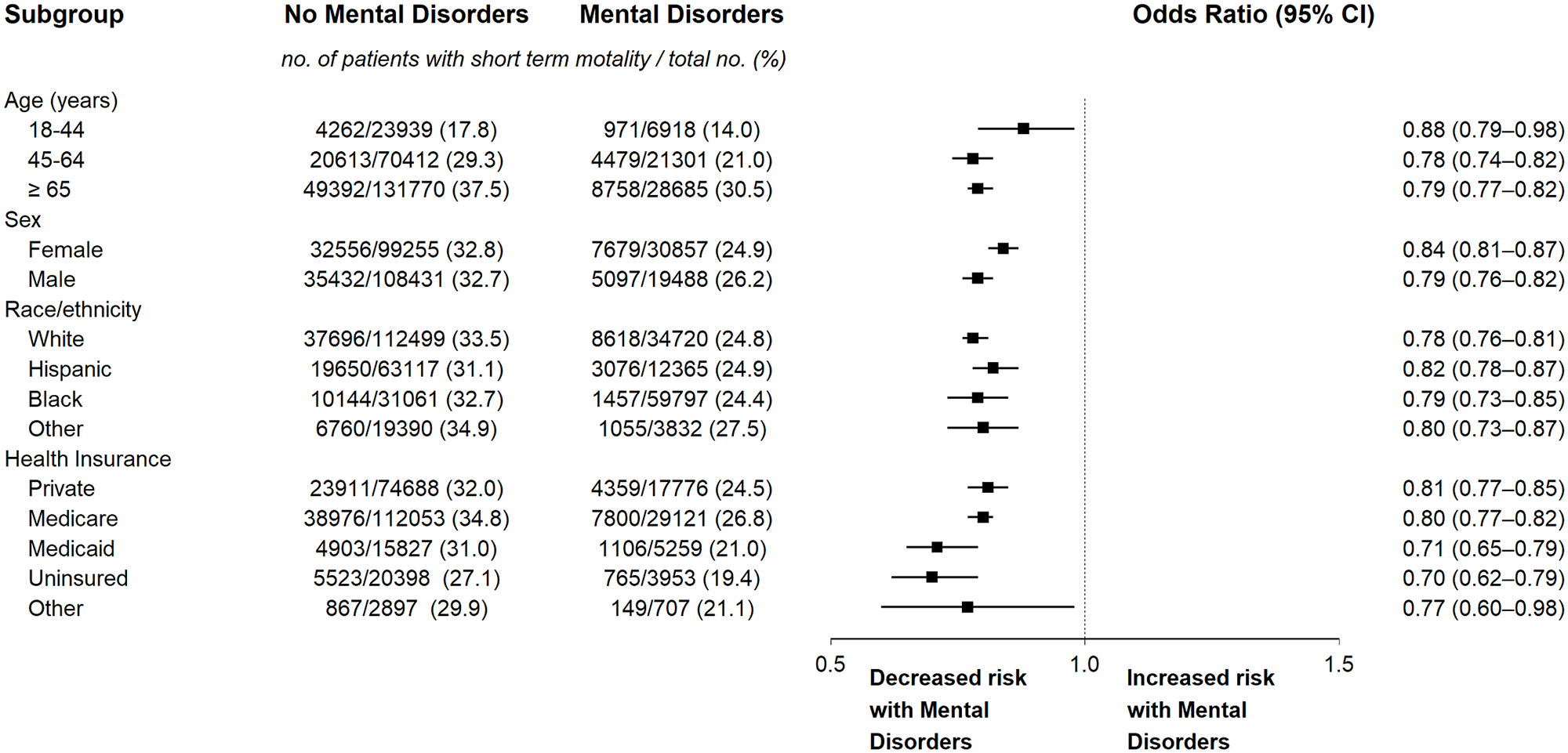
Subgroup analyses of short-term mortality of septic hospitalizations with and without mental disorders.
Analyses were done using multilevel multivariable logistic regression with propensity adjustment. The odds ratios and 95% confidence intervals have not been adjusted for multiplicity and should not be used to infer definite effects. show less
Discussion
Key findings
In this population-based study, presence of mental disorders among patients with sepsis was associated with 21% lower risk of short-term mortality. This finding was robust across 3 distinct modeling approaches, as well as within subgroup analyses, with similarly consistent findings within individual categories of mental disorders.
Relationship to previous studies
It was our hypothesis that the many health-related challenges faced by patients with mental disorders, outlined earlier, will increase their risk of death following sepsis. However, our analyses showed, unexpectedly, that presence of mental disorders was associated with reduced risk of short-term mortality in a large sepsis cohort. Although our findings are concordant with other studies from Germany [21] and the US [22, 23], more detailed comparisons are precluded by lack of data on the characteristics of septic patients with and without mental disorders in these reports.
The sources of the contrasting findings between our cohort and the increased short-term mortality among septic patients with mental disorders in the studies from Denmark are unclear. The Danish studies reported only the characteristics of infected hospitalized patients with and without mental disorders, but not those of the subgroup with sepsis [19, 20]. Infected patients with mental disorders in these latter studies were older and had higher burden of chronic illness than those without these conditions. It is unlikely that the subgroup of septic patients with mental disorders in these studies were younger and healthier than those with infections in general. By contrast, the favorable outcomes among patients with mental disorders in our study could be explained by their younger age and lower comorbidity burden compared to those without mental disorders, as well as by their higher frequency of white race, as racial and ethnic minority status is associated with higher mortality in sepsis [4]. However, the lower risk of short-term mortality among sepsis hospitalizations with mental disorders in our cohort remained following addressing these groups imbalances on risk-adjusted analyses. On the other hand, although the increased risk of short-term mortality among septic patients with mental disorders in the Danish studies remained on adjusted analyses, the investigators did not report on, nor adjust their analyses for measures of illness severity or organ support [19, 20], which could further explain the observed outcome differences across studies. Nevertheless, we cannot exclude the possibility that differences between the populations of US and Denmark beyond those captured in cohort characteristics and analytical methods may have contributed to the differences in the prognostic impact of mental disorders between our cohort and the Danish studies.
Notably, the presence of more favorable demographic and clinical characteristics among patients with mental disorders was not associated with more favorable outcomes in studies that did not focus on sepsis. In two recent studies that evaluated the prognostic impact of mental disorders in a heterogenous population of medical and surgical critically ill patients in the US, the groups with mental disorders were, similarly to our cohort, younger, more commonly white, with lower burden of comorbidities, and had lower illness severity [43, 44]. However, on adjusted analyses, mental disorders were associated with either no prognostic effect [43] or higher 30-day mortality [44]. Indeed, in numerous other studies of the prognostic implications of mental disorders in hospitalized patients where sepsis was not the condition of interest, presence of mental disorders had no prognostic advantage, but was rather associated with higher risk of death [45–49].
The mechanisms underlying the lower risk of short-term mortality associated with mental disorders among septic patients are unclear. Two potential contributors may be considered for the favorable outcome associations observed in the present study and in prior reports.
First, the response to infection could have differed in patients with mental disorders who progressed to sepsis, compared to the general population. Several disparate data lines may be linked in the examination of this postulate. Over the past two decades mental disorders were increasingly shown to be associated with immune dysfunction, involving the activation of innate and adaptive cellular effectors [50–52], which is hypothesized to play a causal role in the pathogenesis and clinical expression of these disorders [53–56]. Numerous studies demonstrated systemic low-grade chronic inflammation profile in depression, bipolar disorders, schizophrenia, and in anxiety and personality disorders, characterized by increases in peripheral levels of interleukin-1 (IL)-1 [54, 55, 57–59], IL-6 [54, 55, 57–59], IL-12 [54, 60, 61], interferon-gamma (IFN-γ) [54, 55, 57, 62], and tumor necrosis factor-alpha (TNF-α) [54, 55, 57–59, 61], and decreased levels of IL-4 [54, 58] and IL-10 [54, 55, 62].
Second, recent studies have shown an increased risk of autoimmune disease among patients with depression [63], bipolar disorders [64], schizophrenia [64] and post-traumatic stress disorder [65]. Although the mechanisms for the increased risk of autoimmunity in these populations have not been elucidated, it has been hypothesized that their dysregulated immune state may underlie these observations [63, 65].
Finally, although patients with autoimmune diseases are at an increased risk of infections and sepsis, a recent study by Sheth et al found that among septic patients, those with autoimmune diseases had markedly lower 30-day mortality [66]. On further adjusted analyses, stratified by the level of expression of specific cytokines in autoimmune diseases, 30-day mortality was reduced in those autoimmune diseases with overexpression of IL-1, IL-6, IL-12, IFN-γ, and TNF-α, as well as in those with reduced expression of IL-4 and IL-10 [66]. These associations between pre-sepsis immune dysfunction and mortality are supported by studies showing that sepsis impairs production of IL-1, IL-6, TNF-α [67], IL-12 [68], and IFN-γ [69] and suggesting that this sepsis-induced immunosuppressive state may be augmented by release of IL-4 and IL-10 [69]. The authors hypothesized [66] that patients with pre-sepsis over- and under-expression of specific cytokines may be better suited to survive sepsis-induced impairment in immune function [69–72].
Together, the abovementioned data suggest possible difference in response to infection between those with and without mental disorders, related to the baseline immune dysfunction of the former. However, despite the compelling similarities between the prognostic associations noted in the study by Sheth et al [66] and the cytokine profiles reported in patients with mental disorders, no direct comparative studies of the immune responses of septic patients with and without mental disorders (or those with vs without autoimmune disease) were performed to date. Thus, further studies are needed to both corroborate our findings and to examine sepsis-associated changes across immune function domains in patients with and without mental disorders to further inform strategies to improve sepsis outcomes.
Another potential contributor to reduced short-term mortality among septic patients with mental disorders may be related to the immunomodulating effects of psychotropic agents. Immunomodulating properties of these agents were noted in both in vitro and in vivo studies, though the effects varied across agents and studies [72, 73]. Relatively limited preclinical evidence suggests potentially beneficial effects of psychotropic agents in sepsis. A study of a murine model of septic shock demonstrated decreased mortality following treatment with fluvoxamine [74]. Fluvoxamine is a selective serotonin reuptake inhibitor and a strong agonist of sigma-1-receptor, a resident chaperone protein in the endoplasmic reticulum (ER) [75], acting through inositol-requiring enzyme 1α, which is a major stress sensor in the ER and regulates inflammatory cytokine production [76]. Immunomodulating properties of antidepressants in sepsis were also demonstrated for desipramine, fluoxetine, and amitriptyline, shown to decrease sepsis-induced organ damage [77, 78] and mortality [77] in murine sepsis models, through direct action on expression of inflammatory cytokines. Finally, in another study of murine sepsis, administration of trifuoroperazine, an antipsychotic agent, reduced organ damage and mortality through inhibition of pro-inflammatory cytokine surge, while reducing IL-10 levels [79]. These promising pre-clinical findings are yet to be examined in human sepsis trials. Our data set did not include information on use of psychotropic medications in patients with mental disorders. Further studies of more granular data are needed to examine the association of specific psychotropic therapy and sepsis-associated outcomes among patients with mental disorders.
Study strengths and limitations
Our study has relevant strengths and limitations. In terms of strengths, the present study evaluates a little-examined and important research question and includes a large cohort of consecutive sepsis hospitalizations from an entire population. We adhered closely to reporting guidelines and used statistical methods to limit confounding and enhance trustworthiness in measures of association.
This study has, however, important limitations, in addition to those noted earlier, stemming mostly from use of administrative data and a retrospective design. First, although CCS codes for mental disorders were used in government reports [80] and prior epidemiological studies [81, 82], they were not validated and the optimal ICD-code-based algorithm to identify mental disorders in administrative data has not been determined. Thus, we cannot exclude misclassification between groups. However, misclassification of mental disorders would be expected to blur the differences between groups and thus diminish outcome differences between septic patients with and without mental disorders, leading to possible underestimation of the magnitude of the better outcomes observed among the former. Second, because we could not identify repeated admissions of individual patients in our cohort, it is possible that if the frequency of repeated admissions was higher in the group of patients with mental disorders than among those without these disorders, the denominator for calculation of short-term mortality would have been higher in the former. Such higher denominator could have resulted in erroneously lower estimate of short-term mortality among septic patients with mental disorders, which could not have been addressed on adjusted models. It should be noted, however, that similar methodological limitations affect epidemiological studies in the US based on other deidentified administrative data sets, including the National Inpatient Sample (NIS). However, in a recent study [83] based on the NIS data, that examined the prognostic impact of 3 autoimmune diseases in sepsis (where each of the studied autoimmune diseases is known to be associated with increased risk of sepsis and thus with increased risk of repeated hospital admissions related to sepsis compared to the general population, which could lead in turn to an increased likelihood of artificially lower apparent risk of death among the former, due to the considerations noted above), the risk-adjusted short-term mortality was either higher, lower, or not different among the patients with autoimmune diseases compared to the general population. Nevertheless, we cannot exclude the possibility that repeated hospital admission may have affected our outcome estimates. Third, we did not have information on the severity of mental disorders. In addition, our data set did not include information on processes of care, which may have differed between septic patients with and without mental disorders. Thus, we cannot exclude residual confounding in our models. It should be noted, however, that skewed severity of mental disorders to mostly mild disease would be expected to blur the outcome differences between the examined groups, while skewing toward mostly severe disease would not be expected to result in more favorable mortality outcomes among affected septic patients. In addition, as noted earlier, patients with mental disorders were reported to receive poorer quality of healthcare [10], and stigma, stereotyping, and negative attitudes towards these patients by clinicians have been previously documented [84, 85]. Such care differences would be not be expected, however, to result in better outcomes of septic patients with mental disorders. Fourth, our analyses may not be generalizable to categories of mental disorders not examined in the present study. Last, the generalizability of our findings to other countries and regions, beyond those previously studied, is unknown.
Conclusions
Mental disorders were associated with lower risk of short-term mortality in sepsis. This favorable prognostic association was observed consistently for individual categories of mental disorders and on exploratory subgroup analyses. Additional studies to examine the factors underlying the conflicting across-country prognostic implications of mental disorders are needed to guide future efforts to improve sepsis outcomes.