
Cardiac 11C-Donepezil Binding Increases With Age in Healthy Humans: Potentially Signifying Sigma-1 Receptor Upregulation
By Jacob Horsager, Tatyana D. Fedorova, Nathalie V.D. Berge, Mette W. Klinge, Karoline Knudsen, Allan K. Hansen, Aage K.O. Alstrup, Klaus Krogh, Lars Gormsen, and Per Borghammer
Excerpt from the article published in Journal of Cardiovascular Pharmacology and Therapeutics. July 2019:365-370. doi: 10.1177/1074248419838509
Editor’s Highlights
- Sigma-1 receptors (S1Rs) are upregulated in the heart in response to stress and protects against age-related hypertrophy of the myocardium.
- Age-dependent increase in blood pressure, peripheral resistance, and thus increased impedance, is attenuated by S1R upregulation.
- No other receptor system, transporters, enzymes, or other tracer target molecules in the human myocardium have been shown to increase as a consequence of normal healthy ageing.
- The cardioprotective mechanism of donepezil may be a result of S1R agonism.
Abstract
Background: Donepezil may have cardioprotective properties, but the mechanism is unclear. Using positron-emission tomography (PET), we explored 11C-donepezil uptake in the heart of humans in relation to age. The results are discussed in the context of the cardioprotective property of donepezil.
Methods: We included data from 57 patients with cardiac 11C-donepezil PET scans. Linear regression analyses were performed to explore the correlation between cardiac 11C-donepezil standardized uptake value (SUV) and age. Subgroup analyses were performed for healthy controls, patients with prodromal or diagnosed Parkinson disease (PD), males, and females.
Results: In the total group of 57 patients, linear regression analysis revealed a significant positive correlation between cardiac 11C-donepezil uptake and age (r2 = .63, P < .0001). The average increase was ≈1.25 SUV per decade and a 2-fold increase in SUV from age 30 to 65 years. Subgroup analyses also showed significant correlations: healthy control patients alone (n = 28, r2 = .73, P < .0001), prodromal or diagnosed PD (n = 29, r2 = .28, P = .03), male patients (n = 34, r2 = .49, P < .0001), and female patients (n = 23, r2 = .82, P < .0001). No other organs showed increased 11C-donepezil binding with age.
Conclusions: 11C-donepezil SUV increases robustly with age in the normal human heart. We speculate that the increased donepezil binding is caused primarily by sigma-1 receptor upregulation. If our interpretation is correct, it shows that sigma-1 receptors are dynamically regulated and may represent an overlooked target for pharmacological intervention studies.
Introduction
Donepezil is a reversible acetylcholinesterase (AChE) inhibitor used for symptomatic treatment of Alzheimer disease by increasing acetylcholine (ACh) levels in the brain.1Patients with Alzheimer disease also seem to have a reduced risk of cardiovascular mortality when treated with donepezil.2,3 However, the potential cardioprotective mechanism of donepezil remains poorly understood. Preclinical investigations have shown that donepezil is beneficial as a therapeutic agent in heart failure in rodent models4–7 and suggest that increased levels of ACh by itself may antagonize the hypertrophic effects of an increased sympathetic load (eg, under stress).8–10
However, donepezil also binds to sigma-1 receptors (S1Rs) with comparable affinity to that of AChE.11 The S1R is a chaperone situated in the interface between the endoplasmic reticulum (ER) and the mitochondrion, known as mitochondria-associated ER membrane, and is involved in numerous diseases and physiological processes.12–15 The S1Rs are abundantly expressed in the heart,16 where they are upregulated in response to stress and have protective properties against cardiac hypertrophy.17,18 Thus, a cardioprotective effect of donepezil treatment could be caused by AChE inhibition, S1R binding, or both.
We have recently published a series of in vivo positron-emission tomography (PET) studies in humans using radiolabeled 11C-donepezil as a marker of cholinergic innervation of peripheral organs.19–22 In these study data, we have observed that 11C-donepezil binds quite avidly to the heart and that the binding seemed to increase substantially with age. Furthermore, in autoradiography studies of porcine myocardial tissue, we documented high binding affinity of 11C-donepezil in the low nanomolar range (Kd = 30 nmol/L) and only 16% of total binding was nonspecific.19 However, the relative binding to S1R and AChE was not determined.
Here, we present the cardiac 11C-donepezil PET data from 57 patients without cardiac complaints or history of cardiovascular disease. We discuss the results in the context of the recently suggested cardioprotective properties of donepezil.
…
Results
In all, 57 study patients (23 females, mean age 57, range 24-78) with no history of cardiovascular disease were included (healthy controls = 28, PD = 16 and RBD = 13).
Figure 1 shows 11C-donepezil PET images from a representative young, middle-aged, and aged study patient.
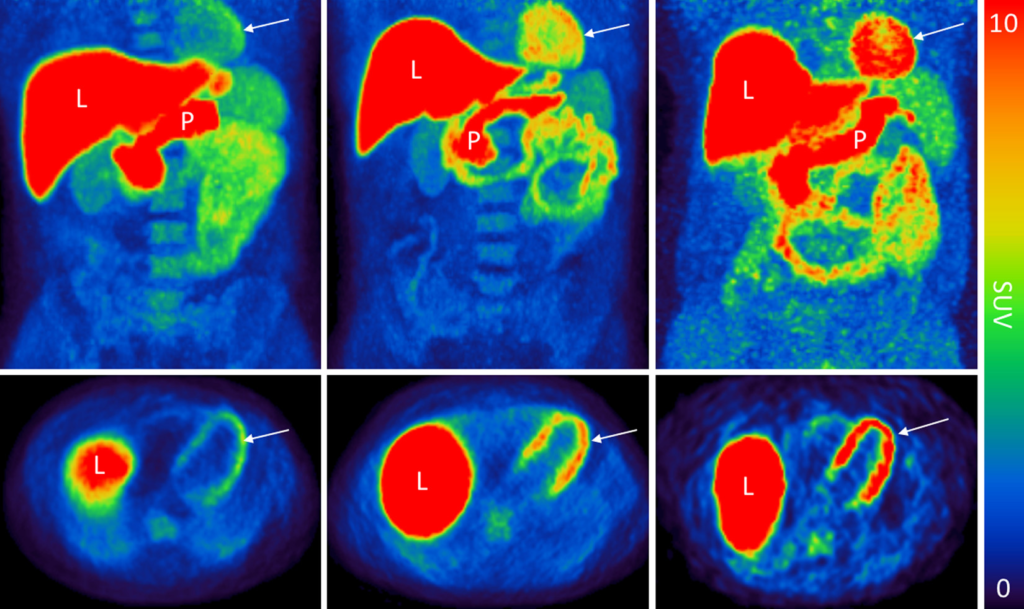
11C-donepezil PET images of 3 representative patients: left column: age 31, middle column: age 53, and right column: age: 73. Top row: maximum intensity projection (MIP) images. Bottom row: transaxial slices. Note the visually apparent increasing 11C-donepezil uptake in the heart (arrows). All images are scaled from 0 to 10 SUV. The 3 patients are emphasized in Figure 2 with gray circles. L indicates liver, P, pancreas; PET, positron-emission tomography; SUV, standardized uptake value.
A highly significant, positive correlation between cardiac 11C-donepezil SUV and age was detected in the total group of 57 patients using a 10-mm brush size (r2 = 0.63, P < .0001, slope = 0.125, Figure 2A). No other organs displayed positive correlations between age and 11C-donepezil SUV. The 11C-donepezil uptake in the pancreas is depicted in Figure 2B (r2 = .006, P = .56).
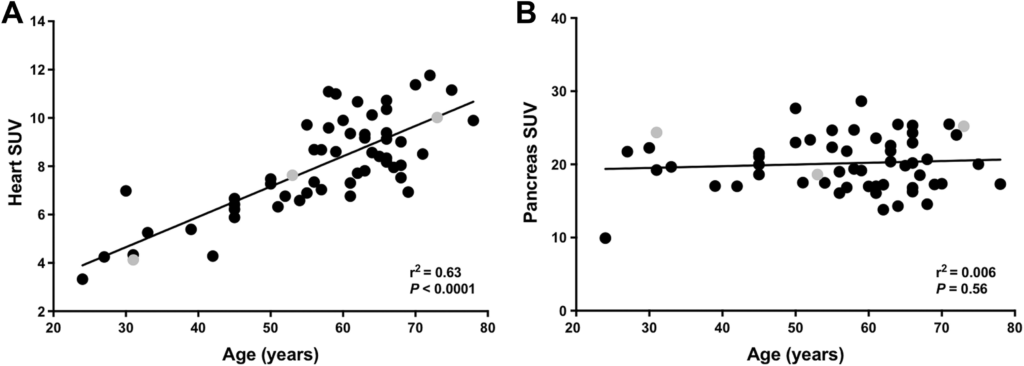
Plots of the heart (A) and pancreas (B) 11C-donepezil SUV in relation to age, presented with the linear regression line (y = 0.125x + 0.9 and y = 0.02x + 18.8, respectively). Gray circles = patients depicted in Figure 1. SUV indicates standardized uptake value.
Subgroup linear regression analyses of cardiac 11C-donepezil data were performed for (1) healthy control patients (n = 28, r2 = .73, P < .0001), (2) cases with PD and RBD (n = 29, r2 = .28, P = .03), (3) male patients (n = 34, r2 = .49, P < .0001), and (iv) female patients (n = 23, r2 = .82, P < .0001). These analyses are graphically presented in online Supplementary Figure 2.
The 16 excluded patients with a history of minor cardiovascular disease was also analyzed and yielded similar results (Supplementary Figure 3).
Multiple linear regression analysis was performed for heart SUV as dependent variable and sex, PD/RBD status (yes/no), and age as independent variables. First, we applied a model allowing for different slopes in each group, but there was no significant interaction on the slope between the groups (P values > .31). Therefore, we could apply a multiple linear regression model with 1 common slope. The slope of the linear regression adjusted for sex and PD/RBD status was 0.13 (r2 = .66, P < .001), mean heart SUV was 0.66 lower in males compared to females (P = .07), and mean heart SUV was 0.29 lower in patients with PD/RBD compared to healthy control patients (P = .42). Sex and PD/RBD status were thus not significant predictors for heart SUV.
The significant positive correlation with age was robust when using the progressively narrow VOIs, sampling only the center of the myocardium (P < .0001 for all analyses; Supplementary Figure 4). The average cardiac VOI volume was 33.7 mL (range 20.4-44.5).
Discussion
In the present study, we observed a significant correlation between age and 11C-donepezil SUV in the human heart. The slope of the linear regression was 0.125, indicating an increase in cardiac SUV of 1.25 per decade and a 2-fold increase in cardiac SUV from approximately 30 to 65 years of age. Subgroup analyses of healthy control patients, cases with PD and RBD, males, and females all showed concurrent significant correlations, underlining the robustness of the result. The positive correlation was also robust across progressively more narrow heart VOIs. Thus, any bias from partial volume effects caused by age-related myocardial hypertrophy was most likely negligible, since the scanner resolution (4.5 mm full-width-at-half maximum) is substantially smaller than the width of the left ventricle myocardium.
In the pancreas, no correlation between age and cardiac 11C-donepezil SUV was observed. In the present context, the important point is that neither the pancreas (Figure 2B) nor any other internal organ (data not shown) exhibits increased 11C-donepezil uptake with age, whereas age-dependent increase in cardiac 11C-donepezil uptake is extremely robust and of high magnitude. The multiple linear regression analysis revealed that neither sex nor PD/RBD status were significant predictors of heart SUV.
Between-group differences of organ perfusion can impact on SUV values, but a human study found a significant negative correlation between the coronary flow velocity reserve and age.24 Therefore, if anything, we have probably underestimated the true increase in cardiac 11C-donepezil uptake with age. The cardiac SUV has been shown to be an adequate substitute for kinetic modeling.19,20 Therefore, the increased 11C-donepezil SUV most likely reflects an increased density of target proteins for donepezil in the heart, in other words increased density of AChE or S1Rs or both.11
An in vitro study of human heart tissue reported an age-dependent change in AChE-positive nerve density in the conduction system with increasing levels until adulthood followed by a slow decline in the elderly patients.25 Several semiquantitative studies of the AChE innervation density of the myocardium have been conducted, but the results are not consistent; in the new born almost no AChE innervation was observed26 and in 2 studies with different age-groups only sparse and isolated fibers were found.25,27 Another study of young to middle-aged hearts (1-59 years) observed a moderate AChE-positive staining,28and substantial heterogeneity was detected with highest AChE-positive nerve densities in the base and subendocardial parts of the myocardium.29 These studies did not comment directly on any differences between age-groups, and the objective was primarily to evaluate cholinergic innervation of the myocardium and hence with focus on quantifying nerve fibers. However, a nonneuronal, cardiomyocyte-derived ACh machinery (ie, including synthesis of AChE) has recently been described,8,9 and it is unknown whether such cardiomyocyte-derived AChE shows age-dependent changes.
Our previous autoradiography study of porcine hearts showed that 11C-donepezil binds avidly and homogenously across the myocardial muscle,19 which probably have poor cholinergic innervation, as discussed earlier.25–27 It has been reported that parasympathetic innervation of the heart decreases with age,30 and our previous study did not find correlation between cardiac 11C-donepezil uptake and heart rate variability,20 an indirect measure of parasympathetic innervation of the heart. So, if the cardiac increase in 11C-donepezil SUV with age, as seen in this study, actually reflects AChE upregulation, the source is probably cardiomyocytes and not parasympathetic nerve fibers.
However, it is well known that donepezil also binds to S1R with low nanomolar affinity,11 a receptor abundantly expressed in the human heart.16,31,32 The S1R exhibits cardioprotective properties and can stimulate intracellular synthesis of ACh in cardiomyocytes through AChE-independent pathways,10 probably mediated directly through the S1R as shown in neurons.33–35
It has been demonstrated that S1R is upregulated in the heart in response to stress and protects against cardiac hypertrophy.17,18 Moreover, fluvoxamine, a selective serotonin uptake inhibitor and a potent agonist for SR1, attenuated cardiac hypertrophy induced by pressure overload in rats.36 The effect was abolished when the rats were treated with S1R antagonists.36 The same cardioprotective function was achieved by treating ovariectomized rats with dehydroepiandrosterone,37 an endogenous agonist for S1R. It is thus plausible that age-related hypertrophy of the myocardium,23 probably caused by age-dependent increase in blood pressure, peripheral resistance, and thus increased impedance,38 is attenuated by S1R upregulation.
Currently, the cause of the observed, age-dependent increase in 11C-donepezil cardiac binding remains unclear. However, we postulate that it is caused primarily by upregulation of S1Rs for the following reasons: (1) a previous PET study investigated the binding of the S1R ligand 11C-SA4305 in rats and reported 80% higher retention in old rat hearts compared to young,39 (2) a study used polymerase chain reaction (PCR) to quantify the levels of S1R messenger RNA in rat hearts and also showed an age-dependent increase, although this finding fell short of statistical significance,17 (3) evidence from AChE studies using semiquantitative histochemical methods generally suggest that AChE levels in the conducting system decline in the elderly patients and semiquantitative histochemical methods used for myocardium AChE assessment have not reported clear increase with age.25–29
Our study has some limitations. Most importantly, we did not determine exactly which 11C-donepezil target protein increases with age in the human heart. Future studies could utilize the novel and highly selective S1R PET ligand, 18F-FTC-146, and compare cardiac uptake in young and aged patients. Of note, the one available human 18F-FTC-146 study investigated young healthy controls (mean age 34 years) and reported cardiac SUV of ≈4,31 which was comparable with our data (Figure 2A). Also, quantitative molecular techniques, including PCR, and autoradiography analyses with 11C-donepezil and the S1R selective ligand SA4503 as a blocking agent should be applied to studies of human heart tissue from different age groups.
We did not have objective information about the myocardial perfusion status of the patients. Despite the lack of cardiac complaints or history of heart disease, some of our patients could have had silent myocardial infarcts, leading to scar tissue, regionally decreased perfusion, and to decreased cardiac 11C-donepezil mean SUV. This would, however, be much more probable in the aged study patients and would have led to an underestimation of the true age-related increase in 11C-donepezil binding. In the present study, we omitted a regional analysis of myocardial 11C-donepezil uptake because our findings of globally increasing 11C-donepezil uptake with age were very robust. A regional analysis would thus not have contributed significantly to this overall main finding.
To our knowledge, no other receptor system, transporters, enzymes, or other tracer target molecules in the human myocardium have been shown to increase as a consequence of normal healthy ageing. The density of sympathetic nerve terminals, as assessed by 123I-MIBG scintigraphy and 11C-HED PET, remains stable or declines with age.40–42 In contrast, several 11C-methylquinuclidinyl benzilate PET studies have shown that muscarinic cholinergic receptors are upregulated in patients with dilated cardiac myopathy and also in remote nondamaged territories in patients with myocardial infarction.43–45 Thus, cholinergic cardiac receptor upregulation is clearly an adaptive response in several types of heart disease. In the context of the present results, it raises the question whether upregulation of S1R or AChE in the myocardium, as measured by 11C-donepezil PET, is a beneficial adaptive response in elderly patients.
In conclusion, we report a robust positive correlation between 11C-donepezil SUV in the human heart and age. The finding was consistent in groups of control patients and patients with PD and also in males and females in separate groups. The finding can be explained by upregulation of both AChE and S1Rs, although we speculate that the latter is the more probable explanation. The cardioprotective mechanism of donepezil may be a result of S1R agonism or inhibition of AChE or both. Given the striking increase in cardiac 11C-donepezil SUV, future studies should focus on elucidating which of the target proteins is upregulated. This knowledge will potentially shed light on the reported cardioprotective properties of donepezil and, more importantly, could inspire the development of novel therapies to target this biologically important system.